




The immune system provides surveillance and offers protection from pathogenic invaders and prevents detrimental responses against the self that could lead to autoimmunity. Alterations in the innate or adaptive arms of the immune system can lead to immune deficiencies. Persistent lack of adequate immune responses can open the way to chronic inflammatory conditions, which can add another layer of complexity to an already overwhelmed immune system.
Immune disorders versus immune deficiencies
Immune disorders are alterations or dysregulations of components of the immune system, be it in the immune cells or their signaling pathways. These alterations can cause either low- (immune deficiency) or hyper-activity (autoimmunity) of the immune system.
Immune system deficiencies occur when immune responses fail to protect the host against infections.
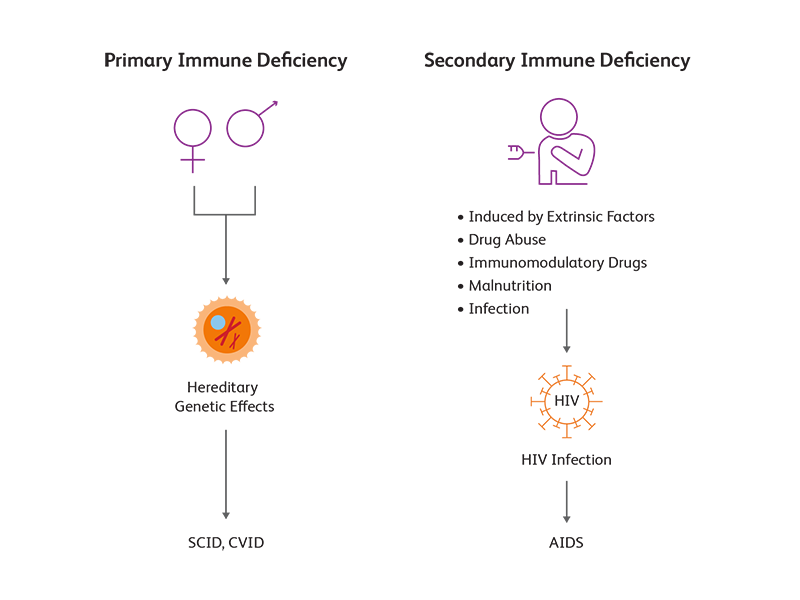
Primary immune deficiencies (PID), such as severe combined immunodeficiency (SCID), occur when some parts of the immune system are absent or deficient. PIDs are usually congenital, deriving from hereditary genetic defects.1
Secondary immune deficiencies (SID) are induced by extrinsic factors in an immune system that is intrinsically competent. Common causes of secondary immune deficiencies include immunomodulatory drugs (e.g., glucocorticoids), malnutrition (e.g., vitamin D deficiency) and chronic infection. Secondary immune deficiencies are more common than primary immune deficiencies; the most prominent secondary immune infection is acquired immune deficiency syndrome (AIDS), which results from infection with human immunodeficiency virus (HIV).
Biology of immune deficiency diseases
Impaired immune cell development results in most immune deficiency diseases. SCID, a PID, is a result of impaired T-cell development, leading to severe T-cell lymphopenia and lack of adaptive immune responses.2 Common variable immunodeficiency (CVID), another PID, is caused by defects in B-cell function and antibody production.3 In AIDS, a SID, HIV specifically infects and reduces the number of CD4+ subset of T lymphocytes.4
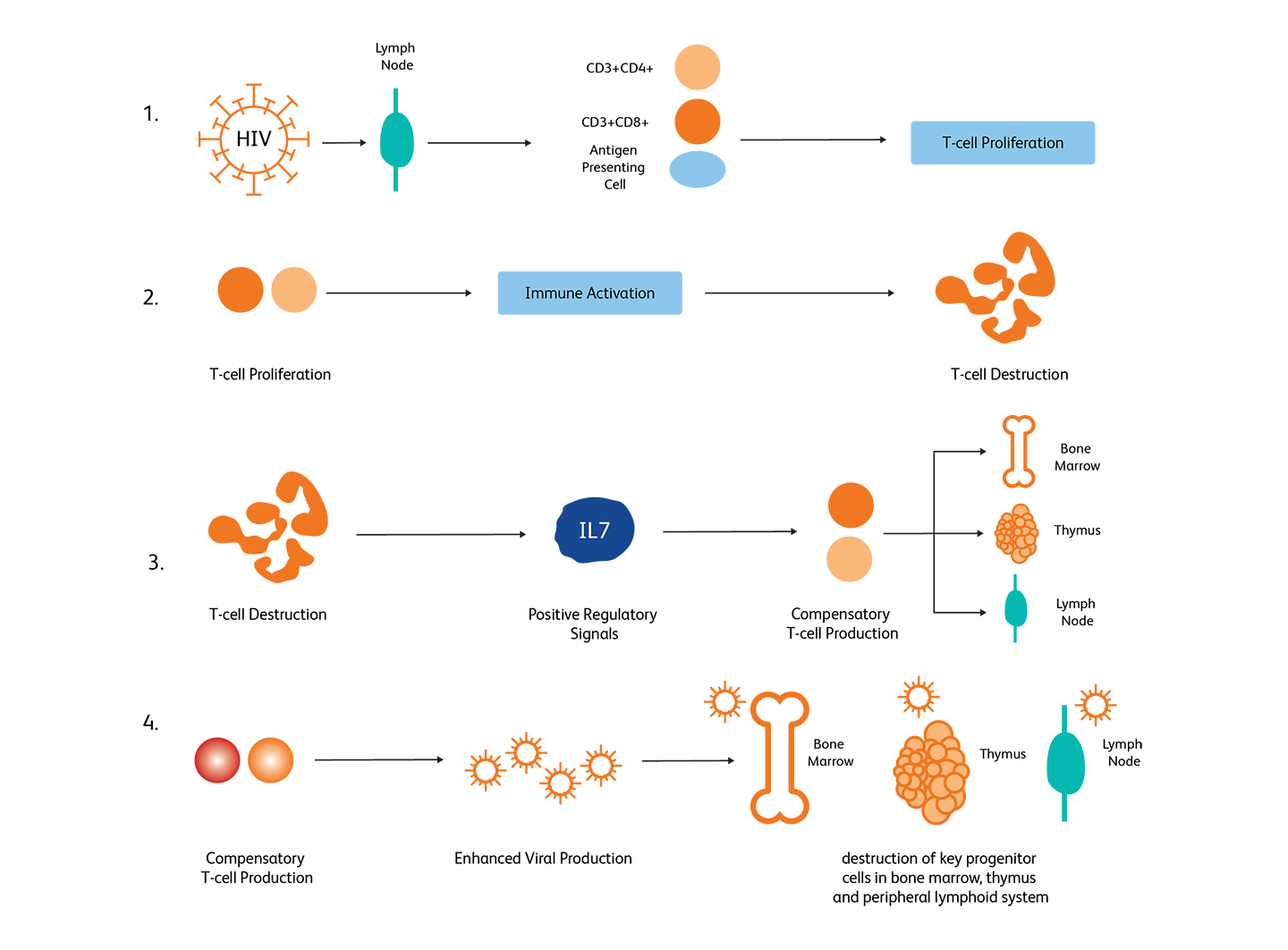
Example of immunodeficiency caused by HIV-mediated CD4+ T-cell depletion. Adopted from McCune, 2001.4
How are immune deficiencies diagnosed?
Immune disorders can be diagnosed either before or after birth depending on the condition:
Prenatal testing
These tests can be conducted using amniotic fluid, blood or cells from the chorion (future placenta).
Blood tests
Collected blood samples can be screened for counts and variety of immune cells and specifically determine the defective cells.
Genetic tests
Targeted sequencing and whole exome sequencing are also used for diagnosis of immune deficiencies, especially for diagnosing newborn SCID.5
Flow cytometry for detecting immune cell types
Flow cytometry is widely used for disease-specific assessments and immunophenotyping of immune cell populations. This evaluation help in diagnosis of immune deficiencies.
BD Biosciences clinical flow cytometry solutions, including instrumentation, software and reagents, offer the building blocks* for laboratory-developed tests used in the identification of markers associated with immune deficiencies.
In addition, the BD FACSLyric™ Flow Cytometry System when used with BD Multitest™ 6-Color TBNK Reagent + BD Trucount™ Tubes offers a clinical solution for immunological assessment of normal individuals, and patients having or suspected of having immune deficiency, with accuracy in cell phenotyping, process efficiency and standardization.
References
- Abraham RS and Aubert G. Flow cytometry, a versatile tool for diagnosis and monitoring of primary immunodeficiencies. Clin and Vaccine Immunol. 2016;23:254-271. doi: 10.1128/CVI.00001-16
- Haddad E, Logan BR, Griffith LM, et al. SCID genotype and 6-month posttransplant CD4 count predict survival and immune recovery. Blood. 2018;132(17):1737-1749. doi: 10.1182/blood-2018-03-840702
- Chinen J, Shearer WT. Advances in basic and clinical immunology 2010. J Allergy Clin Immunol. 2011;127(2):336-341. doi: 10.1016/j.jaci.2010.11.042
- McCune JM. The dynamics of CD4+ T-cell depletion in HIV disease. Nature. 2001;410:974-79. doi: 10.1038/35073648
- Richardson AM, Moyer AM, Hasadsri L, Abraham RS. Diagnostic tools for inborn errors of human immunity (primary immunodeficiencies and immune dysregulatory diseases). Curr Allergy and Asthma Rep. 2018;18(3):19. doi: 10.1007/s11882-018-0770-1
BD FACSLyric™ Flow Cytometers are Class I Laser Products.
The BD FACSLyric™ Flow Cytometer is for In Vitro Diagnostic Use with BD FACSuite™ Clinical Application for up to six colors. The BD FACSLyric™ Flow Cytometer is for Research Use Only with BD FACSuite™ Application for up to 12 colors. Not for use in diagnostic or therapeutic procedures.
*BD Biosciences clinical flow cytometry solutions, including instrumentation, software and reagents, offer the building blocks for laboratory-developed tests used in the identification of markers associated with immune deficiencies. These solutions are not FDA cleared or approved for the diagnosis of immune deficiencies. Analyte Specific Reagent. Analytical and performance characteristics are not established.
23-23019-00